What is being done to combat the inequity seen in NCDs?
It’s clear to see that inequity is rife in regards to NCDs across the globe. As such there have been several key responses that have been implemented by the United Nations (UN) and the World health Organisation (WHO) to combat the inequity seen across the globe in regards to noncommunicable diseases. These strategies have been coordinated by the United Nations interagency task force on the prevention and control of NCDs and are largely operated and controlled by the WHO.
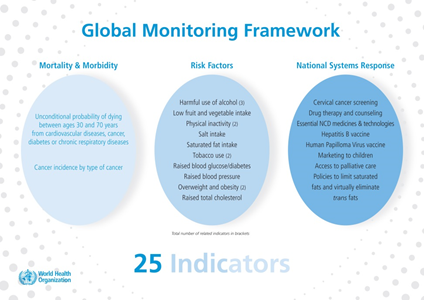
NCD Global Monitoring Framework1
- In 2013, a framework comprising of 9 voluntary global targets and 25 key indicators was presented to member states of the UN.1
- The aim of this framework is to encourage nations to combat mortality associated with NCDs within their own countries.
- The main outcome adopted by the assembly was to reduce NCD associated mortality by 25% by 2025.1

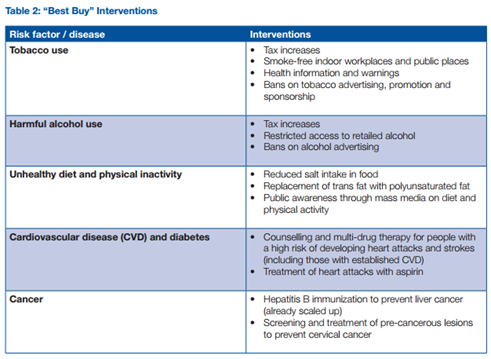
Reducing the economic impact of NCDs in low and middle income countries
- The WHO released a report in 2011 with the aim of addressing the economic problems and inequality associated with NCDs.
- Several risk factors are presented in the report with accompanying cost-effective interventions.
- The total cost for these “best buy” interventions for low income countries stood at US$1 per capita per annum, which constitutes only 4$ of total health expenditure in these countries.2
- These are the potential benefits from the proposed interventional investments:
- Health
- Prevention of around 30 million premature deaths between 2006 and 2015.2
- An average saving of 3 million lives per year.2
- Economics
- A saving of US$25 billion a year.2
- A reduction in economic losses as a result of these diseases of US$377 billion between 2011 and 2025.2
Minor Health Advocacy Organisations
Whilst the activities of WHO are vital for implementation of global change; approaching this issue at a global level means that many individuals remain ignorant of the impact of NCDs within their daily lives. Smaller, local corporations are thus vital to increasing health advocacy at a community level.
EAT
Stordalen Foundation, EAT combines government’s, leading research universities and institutions, philanthropic foundations, non-government actors and organisations to communicate the value of sustainable, nutritious food sources in improve global health. Current goals; including establishing practical guidelines as to the components of a modern health diet; are communicated through global collaborative forums and regionalseminars. In combination with annual presentations; EAT have established a sizable web presence, with an array of educational media being made available.3

SDI
Dwellers International (SDI) are an association of community-based
organisations serving to combat the cost of urbanisation of those within
developing nations within Africa, Asia and Latin America. They provide locals
with the tools to improve their living environment. Assisting their engagements
with local authorities and governing powers; to survey local communities and generate
detailed development plans based on the local socio-economic profiles. Organisation of developments in this manner means that they remain sustainable; properly facilitated and safe to live in. Examples of current projects include housing an infrastructure upgrading in Peru and the Nungua Zongo Communal Water Project.4

organisations serving to combat the cost of urbanisation of those within
developing nations within Africa, Asia and Latin America. They provide locals
with the tools to improve their living environment. Assisting their engagements
with local authorities and governing powers; to survey local communities and generate
detailed development plans based on the local socio-economic profiles. Organisation of developments in this manner means that they remain sustainable; properly facilitated and safe to live in. Examples of current projects include housing an infrastructure upgrading in Peru and the Nungua Zongo Communal Water Project.4
NCD Free
A local organisation, NCD free are a growing voice within the global media. Publishing articles within The Age and PLOS their current aim in to increase global awareness of thecontributing factors in NCD development. Informing readers as to the effect of
diet, alcohol, tobacco use and exercise on disease development; their message
is targeted towards all socioeconomic groups. Importantly NCD free are trying
to abolish the misconception that NCDs only affect those in first world
countries. In fact the majority of their recent publications have been
emphasized the role of NCDs in LMIC’s.

Instagram means that they are in constant communication with their audience.5
The link below gives a brief over view of their approach to health advocacy
https://player.vimeo.com/video/100172370
So what else needs to be done?
These strategies are a step in the right direction in combating the growing problem of inequity in NCDs; however it’s clear that we need to do more.
1. There needs to be a global increase in public awareness of both the causes and the extent of the problems associated with NCDs, particularly in low and middle economic countries (LMIC). Education plays a vital role in controlling many of these diseases and as such more input is needed from governments to assist people in learning about preventing and managing the problem. Simply increasing input into anti-smoking and healthy eating campaigns in LMICs would be a great start.
2. Although health spending in developing countries has tripled in recent years6, a huge gap remains between what is being provided and what is necessary. This is particularly true in the case of NCDs, with only a small fraction of health expenditure being placed in this area.6 Additionally, funding for NCDs currently sits at a mere 1.2% of the international financial assistance provided via the Development Assistance for Health (DAH).7
3. It is also apparent that the importance of the targets set under the WHO action plan are not being emphasised enough. Although the framework is having a positive impact on the issues associated with NCDs, the voluntary nature of the targets makes it difficult to monitor and enforce them. The framework needs to be more stringently enforced and include compulsory aspects of each target that must be undertaken by nations.
References
1. Global action plan for the prevention
and control of noncommunicable diseases [Internet]. Geneva: World Health
Organization; 2013 [cited 2015 Apr 7]. NLM classification: WT 500. Available
from: http://apps.who.int/iris/bitstream/10665/94384/1/9789241506236_eng.pdf
2. From Burden to “Best Buys”: Reducing the Economic Impact of Non-Communicable Diseases in Low- and Middle-Income Countries [Internet]. Geneva: World Health Organization; 2013 [cited 2015 Apr 7]. Available from: http://www.who.int/nmh/publications/best_buys_summary.pdf?ua=1'
3.EAT Forum [Internet] 2013 [updated 2015 April 8; cited 2015 Apr 9]. Available from: http://www.eatforum.org/
4.Shack/ Slum Dwellers International [Internet] 2009 [updated 2015 March 25; cited 2015 Apr 9]. Available from: http://www.sdinet.org/about-what-we-do/
5.NCD Free [Internet] 2014 [updated 2015 April 8; cited 2015 Apr 9]. Available from: http://ncdfree.org
6. Health at a Glance 2013: OECD Indicators [Internet]. Paris: OECD Publishing; 2014 [cited 2015 Apr 7]. Available from: http://dx.doi.org/10.1787/health_glance-2013-en
7. Financing Global Health 2013: Transition in an Age of Austerity [Internet]. Seattle: Institute for Health Metrics and Evaluation; 2014 [cited 2015 Apr 7]. Available from: http://www.healthdata.org/sites/default/files/files/policy_report/2014/FGH2013/IHME_FGH2013_Full_Report.pdf


.jpg)


{kind=link}